 1.855.305.2430
1.855.305.2430
Lactose Intolerance Genes: Understanding Your Dairy Sensitivity Leave a comment
Key Takeaways
- Lactose intolerance is primarily determined by genetic variants in the MCM6 and LCT genes, which control your body’s production of the lactase enzyme
- About 68% of the world’s population has lactose intolerance, with rates varying significantly based on ethnic background and geographical ancestry
- The ability to digest lactose into adulthood (lactase persistence) is actually a genetic mutation that evolved as humans began dairy farming about 10,000 years ago
- Primary lactose intolerance is inherited in an autosomal recessive pattern, meaning you need to inherit the gene variant from both parents to develop symptoms
- While genetic testing can determine your lactose tolerance genes, your actual symptoms may vary based on gut microbiome, inflammation, and other digestive factors
That dairy discomfort you feel isn’t just in your head—it’s in your genes. If milk and cheese leave you bloated, cramping, or running to the bathroom, your DNA might be to blame. Lactose intolerance affects approximately 68% of the global population, making it more common than the ability to digest dairy comfortably. Healthline, a trusted resource for digestive health, explains that what many consider a disorder is actually the genetic norm for adult humans.
The science behind dairy digestion comes down to a specific enzyme called lactase. This enzyme breaks down lactose (milk sugar) into simple sugars your body can absorb. Without enough lactase, undigested lactose passes into your colon, where gut bacteria ferment it—causing the classic symptoms of gas, bloating, and diarrhea that lactose-intolerant individuals experience.
What Happens When You Eat Dairy
When you consume dairy products, you’re ingesting lactose, a disaccharide sugar composed of glucose and galactose molecules bonded together. In lactose-tolerant individuals, the lactase enzyme immediately breaks this bond, allowing these simple sugars to be absorbed through your intestinal wall. However, if you lack sufficient lactase, the undigested lactose acts as food for your gut bacteria, which produce gas as they feast. Additionally, this unbroken lactose draws water into your intestines through osmosis, resulting in diarrhea.
The severity of your symptoms depends on several factors: how much lactase you produce, the amount of dairy consumed, and even the specific composition of your gut microbiome. Some people experience mild discomfort after a large ice cream serving, while others suffer intense pain from just a splash of milk in coffee. This variability makes lactose intolerance a spectrum rather than a black-and-white condition.
Lactose Intolerance vs. Milk Allergy
It’s crucial to understand that lactose intolerance is not an allergy. While they may share some similar symptoms, these conditions involve completely different mechanisms in your body. Lactose intolerance is a digestive issue caused by insufficient enzyme production—your immune system isn’t involved. A milk allergy, by contrast, triggers an immune response to milk proteins (usually casein or whey), potentially causing more severe and even life-threatening reactions. To learn more about how genetic factors can influence your health, you might find it helpful to read about how your genes influence your health.
Milk allergies typically appear in early childhood and often resolve with age, while primary lactose intolerance usually develops later in life. The distinction matters because management strategies differ significantly. While someone with lactose intolerance might tolerate small amounts of dairy or benefit from lactase supplements, these approaches won’t help—and could be dangerous—for someone with a true milk allergy.
The MCM6 and LCT Genes: Your Dairy Digestion Controllers
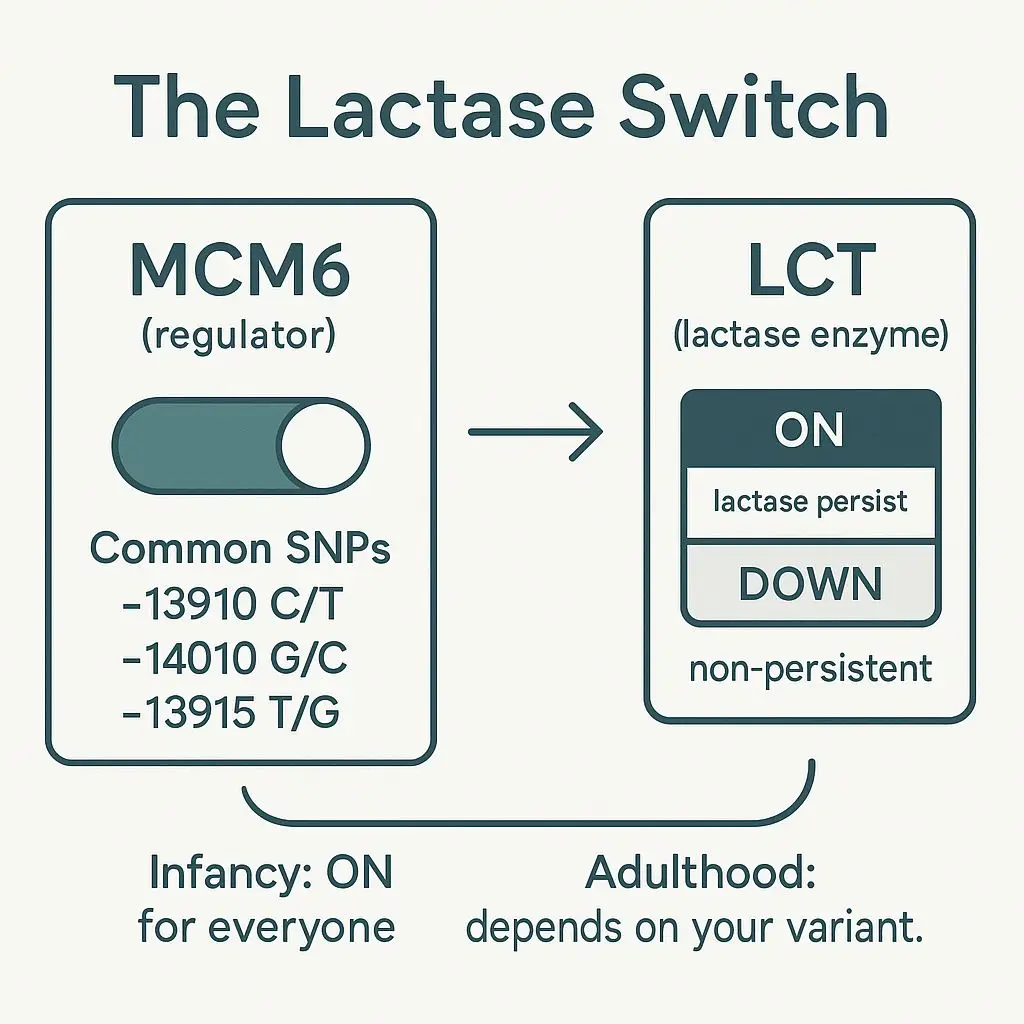
Your ability to digest dairy hinges primarily on two genes: LCT and MCM6. The LCT gene contains instructions for producing the lactase enzyme, while the MCM6 gene controls when and how much lactase your body makes. These genes work in tandem, functioning like a factory (LCT) and its management team (MCM6).
Genetic testing reveals that certain variations in these genes determine whether you’ll maintain lactase production throughout adulthood. These variations developed in human populations that domesticated dairy animals thousands of years ago, providing a nutritional advantage in times of food scarcity.
How the LCT Gene Works
The LCT gene sits on chromosome 2 and contains the complete instructions for building lactase enzymes. This gene is active in the cells lining your small intestine, where lactase is needed to break down the lactose in your diet. Every human is born with a functioning LCT gene—this makes evolutionary sense because all mammals, including human infants, rely on milk as their primary food source.
What makes lactose intolerance interesting from a genetic perspective is that the LCT gene itself rarely contains mutations. Instead, it’s the regulation of this gene that changes over time. In most mammals and historically in humans, the activity of the LCT gene naturally decreases after weaning, as milk is no longer needed in the diet. This downregulation is the default genetic programming for humans.
The MCM6 Gene’s Regulatory Role
The MCM6 gene is the true mastermind behind lactose tolerance or intolerance. Located just upstream from the LCT gene on chromosome 2, it contains crucial regulatory elements that control LCT gene expression. Think of MCM6 as the on/off switch for your lactase production.
“The ability to digest milk as an adult evolved multiple times independently in different human populations, each time through changes in the MCM6 gene that kept the LCT gene switched on throughout life. This represents one of the strongest examples of recent natural selection in humans.” — Genetic Science Learning Center, University of Utah
The fascinating aspect of lactose tolerance is that it evolved through different mutations in the MCM6 gene across various populations. Europeans, Middle Easterners, and some African populations all developed lactase persistence independently, but through different genetic changes—a perfect example of convergent evolution in humans.
Single Nucleotide Polymorphisms That Determine Dairy Tolerance
The specific genetic variations that allow adults to digest lactose are single nucleotide polymorphisms (SNPs) within the MCM6 gene. These tiny changes—where just one letter in the genetic code is altered—can have profound effects on lactase production. The most well-studied variant is C/T-13910, which is common in European populations. If you have the T allele rather than the C allele at this position, you’re likely to maintain lactase production into adulthood. For more information, you can explore the genetics of lactose intolerance.
Other populations have different SNPs associated with lactase persistence. In East Africa, variants like G/C-14010 and T/G-13915 emerged independently, allowing pastoral populations to thrive on dairy-heavy diets. These diverse genetic adaptations highlight how important milk consumption became in certain human populations, strong enough to drive parallel evolutionary changes.
Lactase Persistence: The Genetic Mutation That Let Adults Drink Milk
The ability to digest lactose beyond infancy is actually the genetic anomaly, not the inability. Lactase persistence—continuing to produce lactase enzymes into adulthood—represents one of the clearest examples of recent human evolution. This genetic adaptation appeared only after humans began domesticating dairy animals roughly 10,000 years ago, making it relatively new in our evolutionary history.
Archaeological evidence suggests that humans were consuming dairy products before they could properly digest them. Early farmers likely processed milk into cheese and yogurt, which have lower lactose content due to fermentation. Over time, random genetic mutations that allowed continued lactase production provided a survival advantage, especially in regions where dairy offered crucial nutrition during harsh winters or periods of crop failure.
The Evolution of Dairy Digestion
The timeline of lactase persistence reveals a fascinating story of human adaptation. Genetic studies suggest the European lactase persistence mutation first appeared between 5,000 and 10,000 years ago in central Europe, coinciding with the spread of dairy farming. This mutation then increased rapidly in frequency—one of the strongest signals of positive selection in the human genome.
The independent evolution of lactase persistence in African populations tells a similar story but with different timing and specific mutations. In East African pastoral populations, lactase persistence mutations emerged more recently, approximately 3,000 to 7,000 years ago. This genetic change spread quickly through populations that relied heavily on cattle for sustenance, demonstrating how cultural practices (dairy farming) can drive genetic evolution.
Why Some Populations Can Digest Dairy Better Than Others
The distribution of lactase persistence across human populations isn’t random—it closely tracks ancestral dairy farming practices. Northern European populations show the highest rates of lactase persistence, with up to 95% of people in countries like Sweden and Denmark able to digest lactose comfortably. These high rates reflect millennia of reliance on dairy farming in regions where cold climates limited other food sources.
By contrast, lactase persistence is much less common in East Asian populations, where rates may be as low as 5-10%. This makes perfect evolutionary sense—traditional East Asian cuisines historically contained little dairy, providing no selective advantage for lactase persistence mutations. Similar patterns are seen in indigenous populations of the Americas and Australia, where animal domestication didn’t include dairy species until European contact.
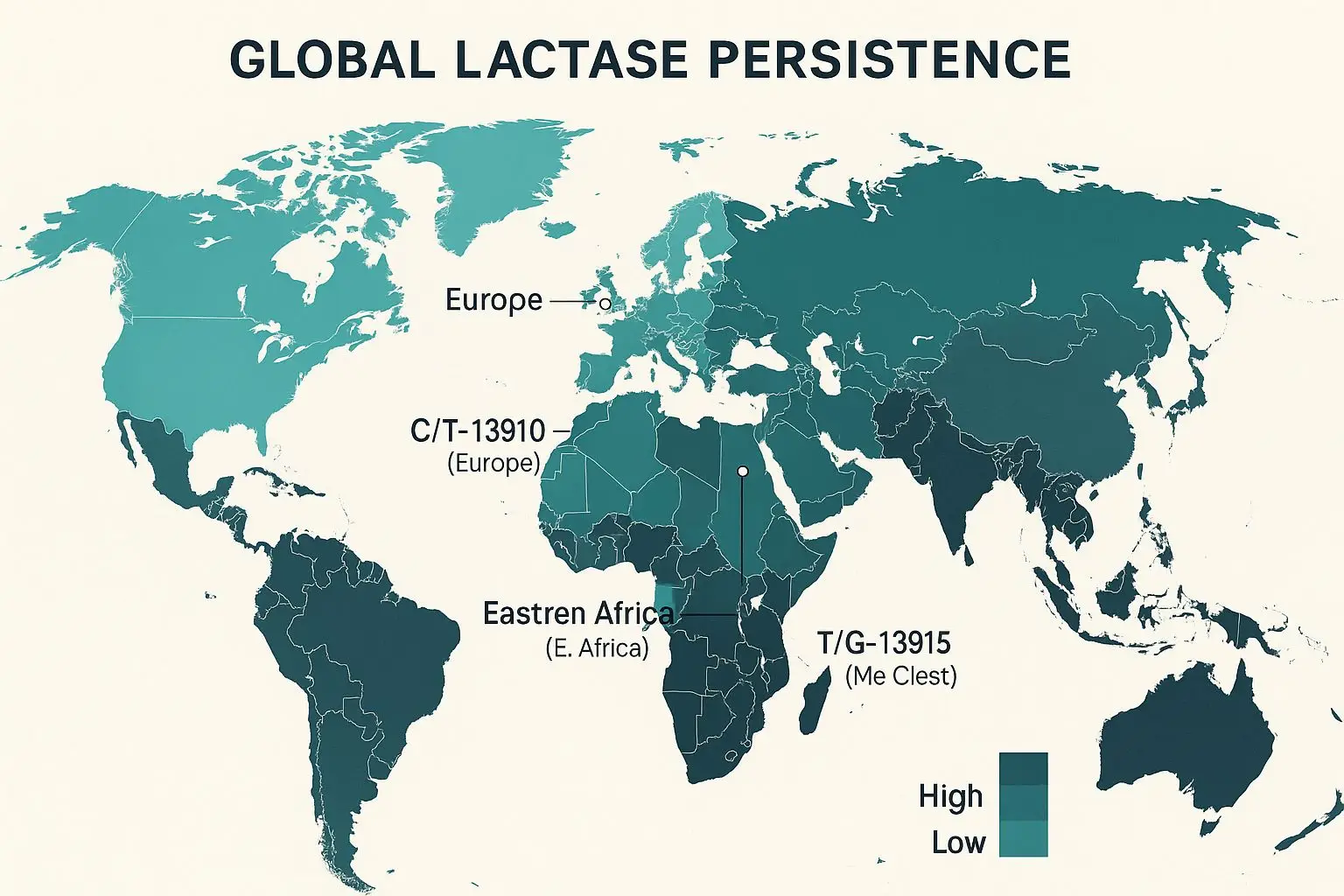
Maps of Global Lactase Persistence
|
Population |
Lactase Persistence Rate |
Primary Genetic Variant |
|---|---|---|
|
Northern European |
85-95% |
C/T-13910 |
|
Mediterranean European |
50-70% |
C/T-13910 |
|
Middle Eastern |
40-70% |
T/G-13915, G/C-13907 |
|
East African |
25-50% |
G/C-14010, T/G-13915 |
|
South Asian |
30-50% |
C/T-13910 and others |
|
East Asian |
5-10% |
Rare, varied |
|
Native American |
10-20% |
Rare, varied |
The 4 Types of Lactose Intolerance
Not all lactose intolerance is created equal. Medical science recognizes four distinct types, each with different causes, development patterns, and genetic implications. Understanding which type affects you can help you better manage your condition and predict how it might change over time. To explore more about the causes and symptoms of lactose intolerance, you can visit the Mayo Clinic website.
Primary Lactose Intolerance: When Your Genes Turn Off Lactase
Primary lactose intolerance is by far the most common form and has the strongest genetic component. This type occurs when your lactase production naturally decreases over time, typically beginning in childhood and becoming noticeable in adolescence or early adulthood. The timing varies significantly between individuals and populations, with some people experiencing a gradual decline in lactase and others facing a more abrupt change.
This form is directly linked to the genetic variants we’ve discussed in the MCM6 gene. If you have the CC genotype at position -13910 (or the equivalent non-persistence variants in other populations), your lactase production is programmed to decrease after childhood. This isn’t a disorder or disease—it’s simply the ancestral human condition, present in most mammals after weaning.
Primary lactose intolerance follows predictable inheritance patterns. Since the lactase non-persistence trait is recessive, both parents must pass down a non-persistence gene variant for a child to develop lactose intolerance. If one parent has lactase persistence (dominant trait), their children will likely maintain the ability to digest lactose throughout life.
Secondary Lactose Intolerance: When Illness Damages Your Gut
Unlike the primary form, secondary lactose intolerance isn’t directly genetic. It occurs when your intestinal lining gets damaged, reducing the lactase-producing cells. This damage can result from gastrointestinal infections, inflammatory bowel diseases like Crohn’s or ulcerative colitis, celiac disease, or treatments like chemotherapy and radiation. The good news is that secondary lactose intolerance is often temporary—once your gut heals, lactase production may recover. To understand how genes influence your health, it is essential to consider both genetic and environmental factors.
Even with secondary lactose intolerance, genetics still plays a role in your recovery. Those with genetic lactase persistence may rebuild their enzyme production more effectively after intestinal damage. For those with genetic non-persistence, an intestinal injury might accelerate the natural decline in lactase that would have happened eventually. This demonstrates how genetics and environment interact to determine your dairy digestion abilities.
Congenital Lactase Deficiency: Born Without the Ability
- Extremely rare genetic disorder (fewer than 50 documented cases worldwide)
- Caused by mutations in the LCT gene itself (not the regulatory region)
- Symptoms begin immediately after birth with first milk feedings
- Requires complete avoidance of lactose, including breast milk
Congenital lactase deficiency represents the rarest form of lactose intolerance. Unlike other types, it results from mutations in the actual LCT gene, preventing the production of functioning lactase from birth. Affected infants develop severe diarrhea upon consuming breast milk or formula containing lactose, which can lead to dangerous dehydration and failure to thrive if not identified quickly.
The disorder follows an autosomal recessive inheritance pattern, meaning both parents must carry a copy of the mutated gene for a child to develop the condition. Most documented cases have occurred in Finland, suggesting a founder effect in that population. With early diagnosis, affected infants can thrive on lactose-free formulas and later transition to a lactose-free diet.
This severe condition highlights the critical importance of the lactase enzyme in early development and explains why evolutionary pressure has maintained functional LCT genes in virtually all human populations, even those where adult lactase production isn’t common. While most lactose intolerance reflects normal human variation, congenital lactase deficiency represents a true genetic disorder.
Developmental Lactose Intolerance: Premature Babies and Lactase
Premature infants sometimes experience temporary lactose intolerance because lactase is one of the last digestive enzymes to develop in the fetal intestine. This type of lactose intolerance usually resolves as the infant matures and is rarely a long-term concern. Special premature infant formulas may be used initially until the baby’s digestive system catches up, though many neonatologists still recommend breast milk for its numerous benefits, even if some lactose isn’t fully digested.
Is Your Lactose Intolerance Hereditary?
If you’re struggling with dairy digestion, family history offers important clues about the genetic nature of your intolerance. Primary lactose intolerance—the most common form—follows clear inheritance patterns that vary by population. Understanding these patterns can help predict whether your children might face similar digestive challenges or whether your symptoms have a genetic basis.
When examining your family tree for lactose intolerance, consider both the presence of symptoms and ethnic background. Some families may not recognize milder symptoms as lactose intolerance, instead attributing them to “sensitive stomachs” or food quality. Additionally, in populations where lactose intolerance is the norm rather than the exception, family patterns may be less obvious since most relatives would share the same genetic predisposition.
Inheritance Patterns of Lactose Intolerance
Primary lactose intolerance follows an autosomal recessive inheritance pattern for lactase persistence, which means the ability to digest lactose as an adult is dominant. If you inherit even one copy of a lactase persistence variant from either parent, you’ll likely maintain the ability to digest dairy throughout life. Conversely, you need to inherit the non-persistence variant from both parents to develop lactose intolerance. This explains why lactose intolerance sometimes seems to “skip” generations or appears unexpectedly in families where dairy consumption has been common.
Why You Might Have It Even If Your Parents Don’t
The recessive nature of lactose intolerance explains why you might develop symptoms even if neither parent seems affected. If both parents are carriers—meaning they each have one lactase persistence gene and one non-persistence gene—they may digest dairy without problems, yet have a 25% chance of having a child who inherits two non-persistence genes and develops lactose intolerance.
Mixed ancestry further complicates inheritance patterns. If one parent comes from a population with high lactase persistence rates (like Northern Europe) and the other from a population where non-persistence is common (like East Asia), their children’s dairy digestion abilities may be unpredictable. The global movement of people and resulting genetic diversity means that family predictions based solely on ethnic background become less reliable with each generation.
Environmental factors can also mask or trigger genetic predispositions. Some people with genetic non-persistence maintain sufficient lactase production well into adulthood due to continuous dairy exposure, gut microbiome composition, or other factors not yet fully understood. Others might have the genetic potential for lactase persistence but develop secondary lactose intolerance due to intestinal damage.
- If both parents are lactose intolerant: Children have nearly 100% chance of developing intolerance
- If one parent is lactose intolerant: Children have varying chances depending on whether the tolerant parent carries a hidden non-persistence gene
- If neither parent is lactose intolerant but comes from typically non-persistent populations: Children still have a significant chance of developing intolerance
Understanding these inheritance patterns helps explain why lactose intolerance can seem unpredictable within families. It also emphasizes why population-level statistics about lactose intolerance prevalence don’t necessarily predict individual outcomes. Your unique genetic inheritance, not just your ethnic background, determines your relationship with dairy.
Genetic Testing for Lactose Intolerance
With advances in genetic technology, you can now discover your lactose tolerance genes without waiting for symptoms to appear. Several testing options—from clinical genetic tests to direct-to-consumer kits—can identify the specific variants in your MCM6 gene that determine lactase persistence. These tests provide insights not just about your current dairy digestion, but also about your evolutionary history and how your genes compare to those of your ancestors.
Genetic testing for lactose intolerance typically examines the key SNPs associated with lactase persistence across different populations. For those with European ancestry, this means testing for the C/T-13910 variant, while those with African or Middle Eastern backgrounds might be tested for additional variants like G/C-14010 or T/G-13915. Most comprehensive tests examine multiple variants to account for diverse genetic backgrounds. For a deeper understanding of how genetic variants can influence health, explore further resources.
- DNA analysis can identify your lactase persistence genotype (CT or TT = lactase persistent, CC = likely intolerant)
- Results provide definitive genetic information but don’t account for secondary factors affecting lactose tolerance
- Testing is available through medical providers or direct-to-consumer genetic testing companies
- Some digestive health panels include lactose intolerance genes alongside other digestive trait markers
While genetic testing offers valuable information, remember that genes don’t tell the complete story of your dairy tolerance. Environmental factors, gut microbiome composition, and even psychological expectations can all influence how you respond to lactose-containing foods. Some people with non-persistence genotypes experience minimal symptoms, while others with the same genetic profile suffer severe discomfort from even small amounts of dairy.
Dealing With Your Dairy Sensitivity Based on Your Genes
Understanding your genetic predisposition to lactose intolerance empowers you to make informed dietary choices. Rather than viewing lactose intolerance as a limitation, consider it an opportunity to explore personalized nutrition based on your genetic makeup. Your genes have evolved over thousands of years to optimize your digestion for certain foods—lactose intolerance simply reflects your ancestors’ dietary patterns.
Managing lactose intolerance successfully requires a combination of self-awareness, dietary adjustments, and sometimes supplements. By tracking your symptoms carefully, you can identify your personal lactose threshold—the amount you can consume before experiencing discomfort. This threshold varies widely among individuals with the same genetic profile, influenced by factors like gut microbiome composition, overall digestive health, and even what foods you consume alongside dairy.
Dairy Alternatives That Match Your Nutritional Needs
The explosion of dairy alternatives in recent years has made living with lactose intolerance easier than ever before. Plant-based milks derived from almonds, oats, soy, rice, and coconut provide options for every taste preference and nutritional requirement. When selecting alternatives, consider not just taste but also nutritional composition—particularly calcium, protein, and vitamin D content, which are key nutrients traditionally obtained from dairy.
Calcium absorption varies significantly between different plant-based sources. For example, calcium from kale and bok choy is highly bioavailable (about 50% absorption rate), while calcium from spinach has poor bioavailability due to its high oxalate content. This is why many plant milks are fortified with calcium in forms specifically designed for optimal absorption.
Protein content is another important consideration when replacing dairy in your diet. While cow’s milk provides about 8g of protein per cup, plant milk alternatives vary widely—from just 1g in rice or coconut milk to 7-8g in soy milk. If you relied on dairy for protein, especially at breakfast, you might need to adjust other food choices to maintain adequate protein intake.
- Soy milk: Highest protein content, complete amino acid profile, moderate calcium when fortified
- Almond milk: Low in protein but naturally contains vitamin E, generally low calorie
- Oat milk: Contains beneficial fiber and often fortified with vitamin D
- Coconut milk: Higher fat content but provides medium-chain triglycerides
- Pea milk: Emerging option with protein content comparable to cow’s milk
Beyond milk alternatives, the market for dairy-free yogurts, cheeses, ice creams, and other traditional dairy products continues to expand. These products increasingly use advanced food technology to mimic the taste, texture, and nutritional profile of their dairy counterparts—making the transition to a low-lactose or lactose-free diet less of a culinary sacrifice than it once was.
Lactase Supplements: Do They Actually Work?
Lactase enzyme supplements offer a way to enjoy dairy occasionally without discomfort. These supplements provide the enzyme your body isn’t producing in sufficient quantities, helping break down lactose before it reaches your colon. The effectiveness of these supplements varies considerably between individuals—likely influenced by the specific genetic variants causing your lactose intolerance, the severity of your enzyme deficiency, and the amount of lactose being consumed.
For best results, take lactase supplements just before consuming dairy products. The enzymes work most effectively when they mix with dairy during digestion rather than being taken long before or after meals. Some people find they need to adjust dosage based on the amount of lactose in different dairy products—a glass of milk contains significantly more lactose than the same volume of aged cheese, for example.
- Tablet forms work well for planned dairy consumption like a restaurant meal
- Liquid drops can be added directly to milk to pre-digest lactose (allowing time before drinking)
- Chewable options offer convenience for unexpected dairy exposure
- Strength varies between brands—experiment to find your effective dose
While supplements can help manage occasional dairy consumption, they shouldn’t be viewed as a complete solution that allows unlimited dairy intake. Even with supplements, your digestive system may still struggle with very large amounts of lactose. Additionally, lactase supplements don’t address potential non-lactose components in dairy that cause sensitivity in some individuals, such as milk proteins or fatty acids.
Building Tolerance Through Small Exposure
Some research suggests that gradual introduction of small amounts of lactose-containing foods might help build tolerance over time. This approach doesn’t change your genetic lactase production but may improve your gut microbiome’s ability to handle lactose. By consuming small, gradually increasing amounts of dairy products (particularly fermented options like yogurt), you might cultivate gut bacteria that more efficiently process undigested lactose, reducing gas production and associated symptoms. This strategy works best when combined with probiotics specifically selected for lactose metabolism support, though results vary considerably between individuals.
Future Treatments for Lactose Intolerance
Emerging research in microbiome modification and gene therapy offers glimpses of future treatments for lactose intolerance. Scientists are exploring targeted probiotic therapies that could enhance lactose metabolism in the gut, potentially reducing or eliminating symptoms without requiring enzyme supplements. These approaches aim to introduce specific bacterial strains that efficiently convert lactose into lactic acid rather than gas-producing byproducts. For those interested in understanding how lifestyle changes can influence gene expression, this research could provide valuable insights.
Even more revolutionary are developments in gene therapy and CRISPR technology that could theoretically activate lactase production by modifying the regulatory regions of the MCM6 gene. While such treatments remain experimental and years from clinical application, they highlight how understanding the genetic basis of lactose intolerance opens doors for innovative solutions. Until then, awareness of your genetic predisposition combined with personalized dietary management remains the most effective approach to living comfortably with lactose intolerance.
Frequently Asked Questions
Lactose intolerance generates many questions about its causes, progression, and management. Here are answers to some of the most common questions people have about the genetic aspects of dairy sensitivity.
Can you suddenly develop lactose intolerance later in life?
Yes, lactose intolerance commonly develops gradually over time rather than appearing suddenly. What seems like a sudden onset is often the culmination of a progressive decline in lactase enzyme production that finally reaches the threshold where symptoms become noticeable. Primary lactose intolerance is programmed in your genes, but the age of onset varies widely—some people notice symptoms in childhood, while others don’t experience difficulties until their 20s, 30s, or even later.
- Genetic factors influence the timing and rate of lactase decline
- Secondary causes like intestinal illness can trigger seemingly sudden intolerance
- Changes in diet or consumption patterns may reveal previously unnoticed sensitivity
- Aging naturally reduces enzyme production in many digestive processes
True sudden-onset lactose intolerance usually indicates secondary lactose intolerance—often following gastrointestinal infection, inflammatory bowel disease flares, or medications that damage the intestinal lining. In these cases, the lactose intolerance may be temporary, improving as the intestine heals. If you experience a sudden change in dairy tolerance, especially accompanied by other digestive symptoms, consult a healthcare provider to rule out underlying conditions.
Interestingly, some research suggests that prolonged avoidance of dairy can reduce lactase production even in people with genetic lactase persistence. This “use it or lose it” phenomenon isn’t fully understood but may explain why some people notice increased sensitivity after eliminating dairy for extended periods. This doesn’t change your genetic capacity for lactase production but may affect enzyme levels temporarily.
If my parents aren’t lactose intolerant, can I still be?
Absolutely. Because lactase non-persistence follows a recessive inheritance pattern, two lactose-tolerant parents can have a lactose-intolerant child if both parents carry a non-expressed gene for lactase non-persistence. This happens because each parent passes one of their two genes to their child, and if both happen to pass the recessive non-persistence gene, the child will develop lactose intolerance even though neither parent shows symptoms. In populations with mixed ancestry or from regions with varying rates of lactase persistence, this genetic “surprise” becomes even more common.
Are there different severity levels of lactose intolerance?
Lactose intolerance exists on a spectrum of severity, with some people experiencing intense symptoms from minimal dairy exposure while others can consume moderate amounts without discomfort. This variation isn’t just psychological—it reflects actual differences in residual lactase production, gut microbiome composition, intestinal transit time, and sensitivity to digestive discomfort. Even among people with identical genetic markers for lactase non-persistence, the amount of lactase actually produced can vary significantly, creating different thresholds for symptom development.
Does lactose intolerance affect all dairy products equally?
Different dairy products contain varying amounts of lactose, which explains why you might tolerate certain dairy foods better than others. Hard, aged cheeses like parmesan or cheddar contain minimal lactose because most is removed during the aging process. Similarly, butter contains very little lactose because it’s primarily fat. Yogurt, especially with active cultures, may be better tolerated because the bacteria partially pre-digest the lactose during fermentation. If you’re curious about how your genes influence your health, understanding lactose intolerance can be an insightful aspect.
Processing methods also affect lactose content. High-fat dairy products generally contain less lactose per serving than their low-fat counterparts. Fermentation reduces lactose content, which is why traditionally fermented dairy products from cultures with high lactose intolerance rates—like Indian paneer or Ethiopian ayib—often have lower lactose levels. Understanding these differences allows many people with lactose intolerance to include some dairy products in their diet while avoiding others that trigger symptoms.
Can children outgrow lactose intolerance if it’s genetic?
Children cannot outgrow primary (genetic) lactose intolerance, as it represents the natural genetic programming for lactase production. What sometimes appears as “outgrowing” lactose intolerance is actually the delayed onset of symptoms—most children naturally produce sufficient lactase throughout early childhood, with decline beginning later depending on their genetic profile. This decline happens at different rates and ages depending on specific genetic variations.
However, children can and often do outgrow secondary lactose intolerance caused by temporary intestinal damage from infection or medication. As their intestinal lining heals, lactase-producing cells regenerate, restoring dairy digestion capacity. The distinction between primary and secondary lactose intolerance becomes crucial here—only the latter type can truly be “outgrown.”
Understanding your genetic lactose intolerance profile doesn’t mean you need to eliminate all dairy forever. By working with your unique biology rather than against it, you can develop personalized strategies that minimize discomfort while maintaining nutritional balance. Whether through careful product selection, enzyme supplements, or dairy alternatives, your genes don’t have to dictate every dietary choice—just inform them. Healthline provides ongoing research and resources to help you navigate dairy digestion based on your genetic makeup.
Lactose intolerance is a common condition that affects many people worldwide. It occurs when the body cannot effectively digest lactose, a sugar found in milk and dairy products. This inability to digest lactose is often due to genetic factors, specifically the presence of certain genes. To better understand how genes can impact your health, you might explore the top 10 genes that impact your wellness journey.
Know your lactose story straight from your genes
Stop guessing and start personalizing. Get clear on your MCM6/LCT status, your true lactose threshold, and the smartest swaps (or supplements) for your biology. Book a genetics-informed nutrition consult with Zenith Vital Wellness.